Most pharmacovigilance (PV) teams treat duplicate literature records as an operational nuisance. A few cases get merged, a few line listings get cleaned up, and the case backlog moves forward. The problem is that this view holds only until an inspector starts asking why the same patient case appears as three separate ICSRs in your safety database, or why your signal counts for a specific product look inflated against EudraVigilance reference data.
At that point, duplicate literature records stop being a housekeeping issue and become a data integrity finding.
The European Medicines Agency itself acknowledges the scale of the problem. Its Medical Literature Monitoring (MLM) service was created specifically to “avoid duplication of effort by marketing authorisation holders” and to “prevent the same reports being entered into databases by multiple marketing authorisation holders” for substances with many authorisations across the EEA. When a regulator builds an entire centralised service to suppress duplicate literature ICSRs, that is a signal worth taking seriously.
This article looks at why duplicate literature records carry real compliance weight, where manual deduplication breaks down, and what defensible literature automation in pharmacovigilance actually looks like under inspection.
Why Duplicate Literature Records Are a Compliance Problem, Not Just a Quality One
The compliance impact of duplicate medical literature records compounds in three directions.
1. Signal detection accuracy
Duplicate ICSRs inflate case counts for specific drug-event pairs. A 2024 analysis published in the Canadian Journal of Physiology and Pharmacology examined literature-derived duplicates in the FDA Adverse Event Reporting System (FAERS) and found that the same published clinical study or case report is often reviewed by multiple companies and reported separately to the FDA, producing a significant population of duplicate records that can lead to false associations between a drug and an adverse event. In disproportionality analyses, inflated case counts directly distort PRR, ROR, and EBGM outputs, generating signal detection false positives that consume investigation cycles.
2. Explicit GVP Module VI obligation
EMA’s Good Pharmacovigilance Practices Module VI (Rev 2) is unambiguous: “literature cases should be checked to prevent the submission of duplicates ICSRs” and “ICSRs are checked in the organisation database to identify literature articles that have already been submitted.” The same module requires that duplicate identifiers be captured in ICH E2B(R3) data element C.1.9.1 (‘Other case identifiers in previous transmissions’) so that downstream merging across senders remains traceable.
3. The audit trail problem
Inspectors do not just look at whether duplicates exist. They look at whether the organisation can demonstrate, with documented evidence, how each duplicate was identified, reviewed, and reconciled. A clean database is not enough if the deduplication process itself is undocumented.
True Duplicate or Follow-Up? The Distinction That Trips Up Manual Review
One of the most common failures in literature deduplication is conflating two cases that look similar but require different actions.
| Scenario | What It Looks Like | Correct Action |
|---|---|---|
| True duplicate | The same patient case republished in a different format (for example, a conference abstract in March, a full journal article in June, a cited case in a review in September). | Merge into a single master case. Capture all source references in ICH E2B(R3) section C.1.9.1. |
| Follow-up report | The same patient case with new clinical information added (revised outcome, additional lab values, updated causality assessment). | Submit as a follow-up ICSR linked to the initial case. Do not merge or nullify. |
| Distinct case, similar profile | A different patient with the same drug-event combination, same age band, and similar narrative phrasing. | Process as a new ICSR. Document the rationale for non-duplication. |
Manual reviewers working through hundreds of weekly hits routinely struggle with this distinction, particularly when narratives are short, anonymised, or translated. AI-based literature screening for drug safety can apply consistent narrative analysis across these scenarios, comparing patient demographics, event timelines, drug exposure data, and reporter identifiers in parallel, then surfacing borderline cases for medical review rather than auto-merging them.
Where Manual Deduplication Workflows Break Down
Most PV teams have a deduplication step in their literature workflow. What they often lack is a deduplication method that holds up across multiple databases and across time.
The DOI-only matching trap
The most common manual approach matches articles on DOI, then on PubMed ID, then on title and author. This works for identical citations. It fails for the cases that matter most:
- Conference abstracts that later appear as full publications carry different identifiers.
- Author name variations across publications (initials versus full names, hyphenated names, transliteration) defeat simple string matching.
- Journal name abbreviations differ between PubMed indexing and Embase indexing, producing parallel entries for the same article.
- Case reports cited inside review articles are often missed entirely, since they appear as references rather than primary entries.
The cross-database overlap problem
GVP Module VI requires literature monitoring across reference databases that contain “the largest reference of articles in relation to the medicinal product properties.” In practice, this means searching PubMed and Embase at a minimum, with regional databases added for products marketed in specific jurisdictions. Each database returns its own version of the same article, which produces duplicate hits at the search-result stage before any case has been validated.
The limit of EudraVigilance's own algorithm
Even centralised duplicate detection has documented gaps. GVP Module VI includes a proven example in which literature-derived case series were submitted by multiple MAHs to EudraVigilance, but because primary source identifiers and patient identifiers were masked, “the duplicate detection algorithm in EV did not identify the reports as potential duplicates.”[3] If the regulator’s own algorithm has known blind spots for literature cases, organisations relying purely on identifier-based matching upstream face the same risk, only without the benefit of EMA-level cross-sender visibility.
What Inspectors Expect From an Audit-Ready Deduplication Process
FDA and EMA inspectors examining literature monitoring do not ask whether you have a deduplication step. They ask whether you can produce evidence of it, on demand, for any case in your safety database.
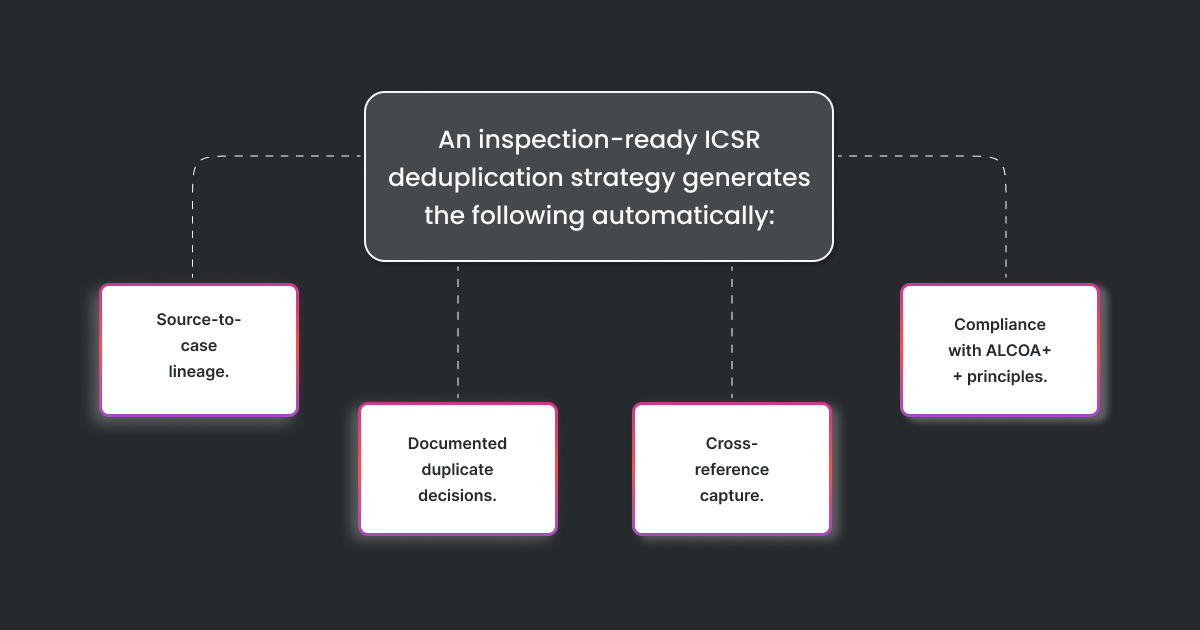
An inspection-ready ICSR deduplication strategy generates the following automatically:
- Source-to-case lineage: Every ICSR derived from literature carries a complete record of which databases were searched, which search strings were executed, which timestamped result set produced the hit, and which version of the article was used for case creation.
- Documented duplicate decisions: For every potential duplicate flagged by the system, the audit log captures the match criteria triggered, the reviewer who validated the decision, the rationale (merge, follow-up, or distinct case), and the timestamp of action.
- Cross-reference capture: Where cases are merged into a master case, the reference numbers of all contributing ICSRs are populated into ICH E2B(R3) section C.1.9.1, in line with GVP Module VI requirements.
- Compliance with ALCOA++ principles: Audit trails for AI-assisted deduplication must meet the same data integrity expectations as any GxP-regulated electronic record under 21 CFR Part 11 and EU GMP Annex 11: attributable, legible, contemporaneous, original, accurate, complete, consistent, enduring, and available.
Manual literature screening logs maintained in spreadsheets, email chains, or paper-based reviewer notes do not meet this standard. Inspectors increasingly expect automated audit trails because the volume and complexity of weekly literature surveillance have outgrown what manual logs can credibly reconstruct.
Clinevo Literature Automation: Built for Deduplication That Holds Up Under Inspection
Clinevo Technologies built its Literature Automation Platform with the assumption that deduplication is a compliance function, not a downstream cleanup task. The platform pulls articles through direct API integration with PubMed and Embase, producing machine-readable, fully logged search results that already meet the traceability expectations of 21 CFR Part 11 and Annex 11.
For deduplication specifically, the platform applies a layered approach:
- Cross-database identifier normalisation reconciles DOI, PubMed ID, and Embase Accession Number variations so that the same article surfaced through parallel searches resolves to a single record.
- NLP-driven narrative analysis compares patient demographics, event timelines, suspect product data, and reporter context across literature cases to identify same-patient publications even when bibliographic metadata differs.
- Confidence-scored duplicate flagging presents high-confidence matches for automated merging and surfaces borderline cases side-by-side for medical reviewer validation, with the audit trail capturing each decision.
- Automated E2B(R3) XML generation populates section C.1.9.1 with cross-references for merged cases, ensuring downstream safety databases and regulatory gateways receive duplicate-aware ICSR records.
The platform also classifies records as ICSR-relevant, PSUR or signal-relevant, or invalid using a curated keyword library combined with text classification models, applying consistent logic across every product and every search cycle. This consistency is what auditors look for when reconciling literature monitoring records against signal management outputs