The first hour of a pharmacovigilance team’s day rarely involves a single, clean stream of cases. It involves audio files from a Medical Information Call Center (MICC) line, scanned MedWatch and CIOMS forms attached to emails, structured submissions from affiliate partners, alerts from a patient support program, literature hits forwarded by the surveillance team, and direct submissions through a consumer portal. Every one of these inputs is a potential Individual Case Safety Report (ICSR). Every one of them carries a regulatory clock the moment it is received.
The volume behind that queue is not slowing down. The European Medicines Agency’s 2025 Annual Report on EudraVigilance shows that 1,765,581 ICSRs were collected and managed in EudraVigilance during 2025 alone, bringing the cumulative database to more than 31.2 million ICSRs covering nearly 17.9 million unique cases. FAERS sits at a similar scale on the US side. And these numbers describe only the cases that reach a regulator. The intake, deduplication, and assessment work that happens inside marketing authorisation holders before any submission is several times large
This is the operational reality that case intake automation in pharmacovigilance must address. Faster typing is not the answer. The answer is a unified intake layer that recognises every source format, extracts the right fields, applies consistent validation, and hands a clean case off to the safety database without manual transcription. That is the design intent behind Clinevo Case Intake.
Why Multi-Source AE Intake Is So Complex
Adverse event reports do not arrive in a uniform shape. A consumer call describing dizziness three days after starting a new prescription is structurally different from a hospital pharmacist’s MedWatch form, which is again different from a patient support program nurse’s structured submission. Each source carries its own gaps, its own language, and its own evidentiary weight.
This heterogeneity creates four persistent operational pressures for PV teams managing multi-source adverse event management:
- Format fragmentation:Some cases arrive as fully structured E2B(R3) XML from partners. Others arrive as a phone recording, an unstructured PDF, or three lines of free text in an email. Without a layer that normalises these into a common case structure, intake teams spend significant time on transcription rather than on medical review.
- Reporter heterogeneity: A 2025 study comparing spontaneous reporting across high-income countries showed that most Canadian reports were submitted by pharmaceutical companies (55%) while UK reports were dominated by healthcare professionals (69%), with direct consumer reports remaining under 10% in both countries. Different reporter types produce unique completeness profiles, and a single workflow cannot treat them identically.
- Under-reporting and missed signals; A separate systematic review cited in the same study found that between 11% and 35% of adverse drug reactions reported by patients are not identified through voluntary reporting by healthcare professionals. If consumer and patient channels are difficult to capture or the data they provide is dropped during intake, real safety information disappears.
- Cost concentration in intake and processing: Case processing is the largest single service segment of the global pharmacovigilance market, accounting for 31.3% of total PV services revenue in 2025.The intake stage sits at the front of that spend, making it the area that either creates or contains most operational waste.
50
New molecular entities cleared by the FDA in 2024. Each approval extends a post-marketing surveillance obligation that the sponsoring organization must maintain indefinitely — expanding workloads without automatic increases in team capacity.
Layered on top of these is a regulatory clock that does not flex. Per ICH guidance and EU pharmacovigilance legislation, fatal or life-threatening unexpected reactions must be reported within 7 calendar days, other serious unexpected reactions within 15 days, and non-serious reports within 90 days for EU post-marketing cases. A case sitting in an unread mailbox over a weekend is not just an inconvenience. It is a compliance event in formation.
Before vs. After
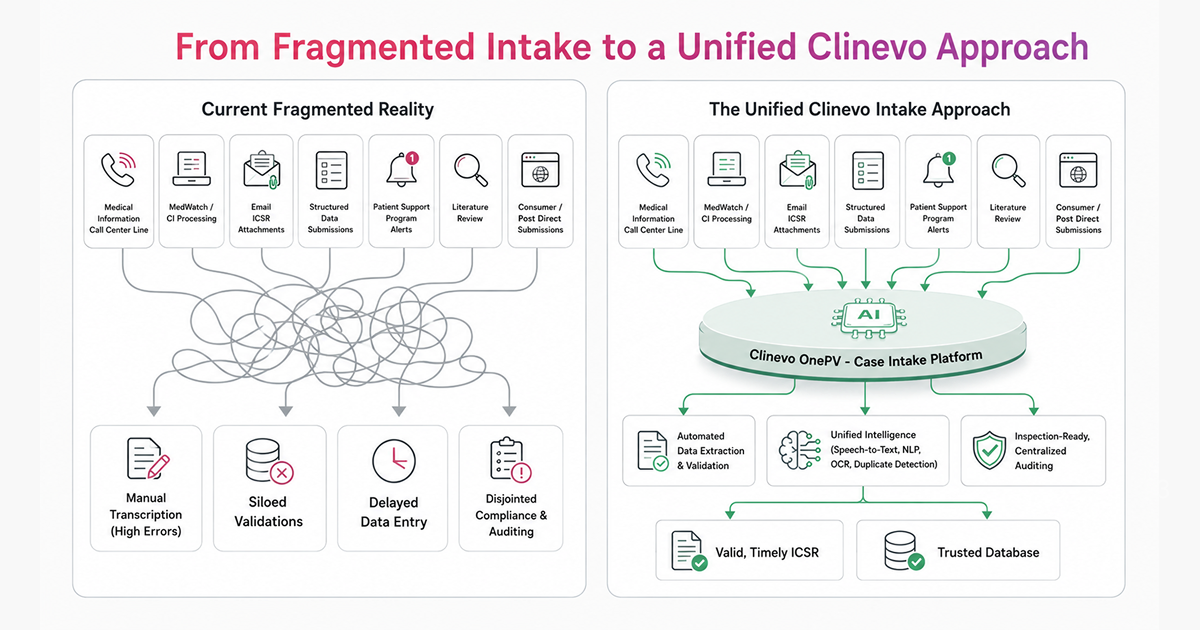
The current state of pharmacovigilance intake is often characterized by a “tangled web” of manual handoffs, where information is re-keyed, validated in silos, and prone to transcription errors at every touchpoint.
As illustrated above, the shift from a fragmented process to a unified intake layer removes the “manual noise.” Instead of teams navigating different portals for phone, email, and portal submissions, the intake layer acts as a standardized processing hub. This visualization represents the core transition: moving from labor-intensive transcription to intelligent, automated data validation.
What an Effective Intake Layer Has to Do
The four pressures above point to the same underlying requirement. Patching a faster front-end onto a fundamentally manual intake process does not solve them. The intake stage itself has to be intelligent at the point of entry, with four design principles holding the workflow together:
- Format normalisation at ingestion : Voice, PDF, email, and structured submissions need to converge into a common case structure before downstream review begins, not as a manual reformatting step afterwards.
- Channel-specific intelligence inside one workflow : The model handling a call recording is not the same as the model parsing a scanned MedWatch form, which is not the same as the rules validating an E2B(R3) submission from a partner. The intake layer has to apply each correctly without forcing the team to switch tools.
- Duplicate detection before database entry:Once a duplicate case sits in the safety database, removing it requires reconciliation work and creates audit complexity. The check has to run at intake, against the connected case repository, before the case is finalised.
- One audit trail across every channel: AI-extracted drafts, human edits, and final validation should resolve to a single inspection-ready record per case, no matter how the case originally arrived.
These principles describe what the intake layer should do. The next question is what implementing them looks like in production.
Inside Clinevo Case Intake
Clinevo Case Intake is built around those four principles. The platform is part of the wider Clinevo OnePV suite and integrates with Clinevo Safety, Clinevo Literature Management, and external safety databases, including Argus Safety, ArisGlobal LifeSphere, and Veeva Vault Safety.
Unified Multi-Channel Intake
The platform consolidates intake from the channels PV teams actually use day to day:
- Telephony and MICC: Voice intake is integrated with AWS Connect, with real-time speech-to-text and structured field capture during the call. The case form populates as the conversation progresses, reducing the post-call documentation gap that typically delays serious case escalation.
- Email and PDF:Inbound emails and attached PDFs (MedWatch, CIOMS I, internal forms) are parsed using NLP trained on PV-specific terminology, with adverse event terms, suspect products, reporter details, and seriousness indicators extracted into structured fields.
- Web portals A consumer-facing intake portal allows direct reporting by patients and HCPs without specialist training, with case-tracking visibility for the reporter once a case is submitted.
- Affiliate and partner submissions:Structured imports from affiliates, distributors, and license partners are ingested through configurable interfaces that preserve the source format for audit purposes.
GenAI-Assisted Field Extraction and Pre-Population
Where Case Intake handles unstructured content, generative AI is used to interpret the report rather than just transcribe it. The model identifies the suspect drug, the adverse event, reporter type, seriousness criteria, and patient demographic data, and pre-populates the case form with confidence scoring against each extracted field. Reviewers focus on validation rather than re-entry, and low-confidence extractions are flagged automatically for human review before they progress.
Multi-Language Identification
The intake layer detects the language of each incoming report automatically. This matters when a single global team is processing cases from EU markets, the UK, Japan, Korea, and India in parallel. Detection happens before extraction, so language-specific NLP routing can be applied without manual triage.
Intelligent Triage and Duplicate Detection
Cases are routed based on seriousness, product, therapeutic area, and jurisdiction. Expedited reports trigger compliance tracking the moment they are validated. Probabilistic duplicate detection runs at intake against existing cases in the linked safety database, so a follow-up arriving by phone is recognised as a follow-up to a case originally received by email rather than entered as a new ICSR. This matters operationally and scientifically. Duplicate ICSRs inflate case counts and distort downstream signal detection in pharmacovigilance.
Compliance Built into the Architecture
Every action in the intake workflow is captured in a tamper-evident, time-stamped audit trail aligned with 21 CFR Part 11 and EU GMP Annex 11 requirements. Electronic signatures are tied to verified user credentials. The audit trail covers the AI-extracted draft, the human reviewer’s edits, and the final validated case. This is the documentation regulators expect to see when they inspect AI-assisted PV workflows. The platform is also GxP-aligned and GDPR-compliant, with controlled processing of personal health data across regions.
AI Transparency and Trust
Adopting Generative AI in a regulated environment requires more than just performance; it requires accountability. We recognize that Chief Information Officers and Regulatory Affairs leaders prioritize data integrity and model fairness above all else. That is why Clinevo Case Intake is engineered with “Human-in-the-Loop” guardrails. We utilize private, isolated AI models that ensure sensitive patient data never leaves your secure environment. Furthermore, our models are continuously validated against a diverse set of real-world PV datasets to monitor for – and mitigate – potential biases in field extraction, ensuring that every reporter type and demographic is captured with the same level of accuracy. AI is an accelerator, but your safety team remains the final authority.
Why a Unified Intake Layer Matters at Scale
The cost case for unified pharmacovigilance workflow automation is well established in industry data. The operational case becomes clearest at intake, because errors and gaps created here compound through every downstream activity. A misclassified seriousness indicator delays expedited reporting. A missed duplicate distorts a signal detection report three quarters later. A mistranscribed product name surfaces during an inspection as a data integrity issue.
Bringing every source into one GenAI-supported intake layer compresses the time from event report to validated case, removes the manual handoffs that introduce most data quality issues, and produces a single audit record that an inspector can follow from the source document through to the submitted ICSR. That is the standard a modern drug safety case intake platform needs to meet.
When to Reassess Your Current Intake Setup
If your team is still copying data from PDFs into safety database fields, if call-derived cases are being documented after the call rather than during it, or if duplicate detection only happens after a case has been entered, the intake layer is doing less than it should be. The clearest signal is where your intake team’s time is going. If most of it is spent on transcription, reformatting, and reconciliation across channels, that is time that should be available for medical review and follow-up.
Frequently Asked Questions
The reliable approach is to consolidate every source, including telephony, email, PDF attachments, web portals, and partner submissions, into a single intake layer that applies consistent extraction, validation, and duplicate detection logic. Without this consolidation, gaps appear at the seams between systems, and that is where data is most often lost. Clinevo Case Intake handles this by ingesting from each channel through one workflow, applying GenAI-assisted field extraction to unstructured inputs, and running duplicate checks against the connected safety database before a case is finalised.
Compliance survives automation when the AI assists, but does not replace, qualified human review, and when every action is captured in a tamper-evident audit trail. Generative AI should handle volume-intensive tasks like field extraction and language identification. Human reviewers should validate extractions, confirm seriousness, and approve the final case. The audit trail should record both layers. Clinevo Case Intake is structured this way, with built-in alignment to 21 CFR Part 11, EU GMP Annex 11, GxP, and GDPR.
Each channel produces a different data format, a different completeness profile, and a different reporter type. A call center recording requires speech-to-text and live structuring. An email with a PDF attachment requires OCR plus PV-specific NLP. A literature article requires assessment against ICSR criteria before any case is created. Treating these uniformly produces gaps. Treating them with channel-specific intelligence inside one unified workflow is how modern intake platforms close those gaps.
Yes, when it is applied to the parts of intake where it has a clear advantage. Generative AI is well-suited to interpreting unstructured narratives, extracting suspect drug and adverse event terms, detecting language, and pre-populating case forms with confidence scoring. It is not a substitute for medical judgment on causality, seriousness, or expectedness. Quality improves because human reviewers spend their time on those judgments rather than on data entry. Clinevo Case Intake reflects this division of work explicitly.
The recurring challenges are inconsistent source formats, duplicate cases generated at the boundaries between channels, language variation across markets, and the lack of a single audit trail spanning the full intake-to-submission pathway. A unified intake platform addresses each of these as a design decision, not as a feature add-on. The integration with downstream systems, including Clinevo Safety, Argus Safety, ArisGlobal, and Veeva Vault Safety, is what allows a validated case to flow through to submission without manual re-entry, which is where most cross-system errors are introduced.